

Symptoms :
- Pain in the abdomen
- Distension
- Loss of appetite
- Nausea
- Vomiting
- Constipation or diarrhea
- Low fever
The human appendix has long fascinated both biologists and physicians. A recent bout of appendicitis has heightened my interest in this organ and has stimulated me to write about it. Because of its small and variable size, an
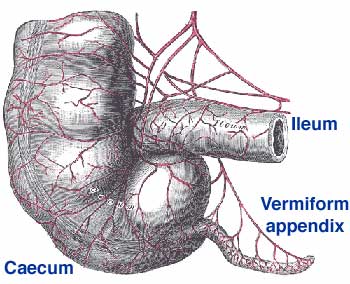
The human vermiform appendix (image from the Talk Origins Archive; www.talkorigins.org)d its apparent uselessness, Darwin (1871) believed that the appendix was a rudiment, or vestigial organ. The caecum is large in many herbivores, in whom it is thought to play a role in the digestion of high-fiber foods. It presumably grew smaller during the course of primate evolution, leaving the appendix as a vestige. Like the rest of the colon, the appendix is rich in lymphatic tissue and its epithelial surface is coated with a biofilm. These properties have led to suggestions that the appendix has been preserved by natural selection because of its immunological functions or because it is a reservoir for commensal bacteria (Bollinger et al. 2007). It seems more likely, however, that these properties simply reflect the development of the appendix as part of the colon; there is little reason to believe that the appendix has unique or especially important immunological or microbiological functions. People who have their appendices removed or who are born with congenital absence of the appendix don’t exhibit any physiological deficits. Darwin was almost certainly correct—the appendix is a rudiment.
If the appendix is a vestigial organ without significant function, and if it can become infected, rupture, and cause death, why has it not been eliminated by natural selection? Nesse and Williams (1994) proposed an ingenious hypothesis to account for the persistence of the appendix. They suggested that small appendices were more likely to become infected and rupture than were large appendices; therefore, mutations that decreased the size of the appendix would increase the incidence of appendicitis and so would decrease fitness. According to this hypothesis, we are stuck at a local fitness peak and can’t evolve to the higher fitness of being appendix-free because of the valley between the peaks. Unfortunately, this hypothesis does not take sufficient account of medical and epidemiological knowledge of appendicitis. A wealth of evidence suggests that appendicitis is a disease of civilization (Kang, Hoare et al. 2003; Bickler and DeMaio 2008).
Although early data on the incidence of appendicitis is limited (the term wasn’t coined until the late 19th century), the available evidence suggests that the disease peaked in developed countries in the early 20th century and has been declining since. The incidence of the disease is much lower in traditional societies and in developing countries than it is in the West, but the incidence is increasing as these countries modernize. The reasons for the changing incidence of the disease aren’t understood but presumably have to do with changes in diet or in exposure to intestinal parasites. Throughout most of human history, appendicitis was probably not an important cause of disability or death. In my view, the Nesse-Williams hypothesis is an elegant solution to a non-existent problem. Again, Darwin was probably right—once a rudiment becomes very small, the cost of maintaining it is minimal and there is little selection to shrink it further.
Nonetheless, people still suffer from appendicitis , inflamed appendices can perforate or rupture (which, fortunately, mine has not), and ruptured appendices can lead to peritonitis and death. How, then, should patients with appendicitis be treated? People have long known from autopsy findings of scarred appendices that some people with appendicitis recover without surgery. Despite this evidence, physicians and surgeons have routinely recommended that patients with appendicitis undergo emergency surgery to forestall perforation. This practice, it seems to me, reflects a lack of appreciation of the strength of our evolved defenses against infection. Moreover, it reflects an essentialist view of disease, in which one of the essential or defining features of appendicitis is progression to rupture. This essentialist notion of disease is inconsistent with an evolutionary understanding of variation. Given that healthy people exhibit variation in virtually all their phenotypic traits, we should expect them to differ in their manifestations of disease. The natural history of appendicitis varies from sub-clinical episodes of abdominal pain to clinically manifest but self-limited infection to infections that lead to rupture. Even among people who have clinical diagnoses of appendicitis, spontaneous recovery is common (Andersson 2006). Surgeons are beginning to appreciate that many patients with appendicitis do not need emergency surgery: some can have surgery on a non-emergency basis, and some can be treated with antibiotics and then have elective appendectomies if their infections recur (Styrud et al. 2006). Some surgeons who cling to an essentialist view of disease have suggested that appendicitis leading to perforation and appendicitis that resolves without perforation are two separate diseases (Søreide 2007). Rational, evolutionarily-sensitive management of patients with appendicitis should recognize the variation in the natural history of this disease. Here as elsewhere, the lesson of evolutionary medicine is that one size doesn’t necessarily fit all.
Treatment :
The diseased appendix must be removed in the acute stage as early as possible .Bibliography
Andersson, R. E. (2006) . The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J Surg 31: 86-92. Bickler, S. W. and A. DeMaio (2008) . Western diseases: current concepts and implications for pediatric surgery research and practice. Pediatr Surg Int 24: 251-255. Bollinger, R. R., et al. (2007) . Biofilms in the large bowel suggest an apparent function of the human vermiform appendix. J Theor Biol. 249: 826-31. Darwin, C. (1871). The descent of man, and selection in relation to sex. London, John Murray. (Freely available from e.g. ebooks@Adelaide or Project Gutenberg ) Kang, J. Y., et al. (2003) . Decline in admission rates for acute appendicitis in England. Br J Surg 90(12): 1586-1592. Nesse, R. M. and G. C. Williams (1994). Why we get sick: the new science of Darwinian medicine. New York, Times Books. (more information on our books page) Søreide, K. (2007) . Should antibiotic treatment replace appendectomy for acute appendicitis? Nat Clin Pract Gastroenterol Hepatol. 4: 584-5. Styrud, J., S. Eriksson, et al. (2006) . Appendectomy versus antibiotic treatment in acute appendicitis. A prospective multicenter randomized controlled trial. World J Surg 30: 1033-1037.






{kind=link}
0 comments